
Three Tests, One Trap
What the ELISA, the Western Blot, and PCR actually measure — and the one diagnostic technique that is never performed

The patient walks out of the clinic with a label. The label will follow him into his insurance file, into his employment record, in some jurisdictions into the criminal docket, and almost always into the next twenty years of his medication regimen and his marriage. The clinician who handed him the label believes it. The patient believes it. The label sounds authoritative because the report from the laboratory sounds authoritative. Antibodies detected. PCR positive. Viral RNA confirmed.
This essay is about what was actually measured.
Three laboratory tests sit at the center of modern infectious-disease diagnosis: the ELISA, the Western blot, and PCR. These same three tests, in various permutations, are used to “diagnose” COVID-19, influenza, hepatitis B and C, HPV, Ebola, MERS, SARS, dengue, Zika, West Nile, malaria, tuberculosis, and HIV. They are increasingly used to “diagnose” cancers — to declare the presence of disease based on an amplified genetic signal rather than on a tumor seen, biopsied, and characterized. The industry says these tests detect proteins, antibodies, and viral or oncogenic genetic material respectively. None of them does what the industry says. The structural failure is the same in all of them: the test measures a physical property of an object, and the disease label is attached to that property by convention. The biology — the question of whether the object whose property was measured is in fact the disease being diagnosed — is never independently verified.
I will use HIV as the working illustration through most of this essay, for one reason: the HIV diagnostic apparatus is the most thoroughly documented example in the world. Decades of litigation, court testimony, package-insert disclosure, peer-reviewed cross-reactivity studies, and the inventor of PCR speaking publicly until his death have placed the receipts on the record. What follows describes the HIV testing architecture in detail, but the same architecture — the same measurement of physical properties, the same conventional attachment of disease labels, the same structural absence of independent verification — runs every infectious-disease diagnosis listed above, and increasingly every PCR-based cancer diagnosis. The HIV literature is just the deepest. The mechanism is the same elsewhere.
The patient is not told this. The clinician is not told this. The package insert of the test itself, in the case of the most widely deployed PCR-based HIV test in the United States, says it plainly. The system runs anyway.
This essay walks through what each of the three tests actually does, what the relevant peer-reviewed literature documents about each, and the one diagnostic technique — the technique by which every major virus of the twentieth century was characterized — that is structurally absent from the workflow.
I. The Western blot: a measurement, not an identification
The Western blot is the cleanest example because the failure is visible in the test’s own nomenclature.
When a patient is told the Western blot revealed antibodies to HIV proteins p24, p17, gp41, and gp120, the patient hears the language of identification. He assumes that named molecular entities, characteristic of a specific virus, have been found in his blood. That is not what the laboratory has done.
The designation p24 does not name a particular protein. It names a band on a gel — specifically, a band whose migration distance corresponds to a molecular weight of approximately twenty-four kilodaltons — abbreviated kDa (a Dalton is the unit of molecular mass in chemistry and biology, equal to one-twelfth the mass of a carbon-12 atom; one kDa equals one thousand Daltons). The lowercase p stands for protein. The number stands for the protein’s approximate mass in kDa. Together they describe one physical property of an object: how heavy it is. That is the entire content of the measurement.
The diagnosis HIV-positive is then attached to that weight, by convention, written into a lab manual. The band at the 24 kDa position is called HIV p24. The naming is the only thing tying that band to the alleged virus.
Imagine a police officer who tells the court he has identified a robbery suspect by weight alone. He places the suspect on a bathroom scale, reads 175 pounds, and announces: that is the man we want. The scale is calibrated. The reading is real. None of that is in dispute. What is in dispute is whether a single number on a scale can identify one human being in a city of millions, when tens of thousands of other men weigh exactly the same amount. No competent court would accept the identification.
Weight is a property. It is not a fingerprint. It is not a face. It is not a name.
The HIV Western blot operates on the same logic, with the same defect. The gel separates proteins by molecular weight — one property, measured along one axis. A band appears at the 24 kDa position. The test announces: that is HIV p24. But a 24 kDa band, like a 175-pound man, is a coordinate shared by an enormous number of unrelated candidates. Human cells produce on the order of 20,000 distinct proteins, and the relevant mass range of a Western blot — roughly 10 to 200 kDa — contains, on average, dozens of distinct human proteins in every 1 kDa interval before fragments, glycoforms, and contaminants are counted. The 24 kDa band is shared by human transaldolase, several histone variants, ribosomal L13a, immunoglobulin light-chain fragments, and a long list of less-characterized cellular species. The 41 kDa position — gp41 in the test’s nomenclature — overlaps with actin, the most abundant protein in every human cell. The 66 kDa position overlaps with albumin, the most abundant protein in human serum.
The Western blot has no second property with which to distinguish a named HIV band from any of those confounders. No sequencing step. No mass-spectrometric confirmation. No antibody specificity control against a purified reference protein. No functional assay. The identification of the band as HIV p24, or gp41, or gp120, rests on one measurement — the band’s position on the gel — and on the manufacturer’s instruction that a band at this position is to be reported as this HIV protein. The detective has identified the suspect by weight. The lab has identified the protein by mass. The structural error is the same.
The same is true of every named band on a Western blot:
p7 — a protein at approximately 7 kDa
p17 — a protein at approximately 17 kDa
p24 — a protein at approximately 24 kDa
p31 — a protein at approximately 31 kDa
gp41 — a glycoprotein at approximately 41 kDa
p51 / p55 / p66 — proteins at the corresponding weights
gp120 / gp160 — glycoproteins at the corresponding weights
The letter g denotes a glycosylated protein. The numbers are masses. Nothing in the nomenclature, on its face, identifies any of these bands as belonging to HIV rather than to any other source of protein of comparable molecular weight.
II. What the laboratory operator actually sees
The Western blot procedure produces a nitrocellulose strip on which serum proteins have been separated by molecular weight, transferred from a gel, and reacted with the patient’s serum. Where the patient’s antibodies bind to a protein on the strip, a colored band appears. The operator examines the strip, records the band positions, and reports them by molecular weight.
The operator does not see HIV. The operator does not see viral particles. The operator does not even see proteins in any morphological sense. The operator sees colored marks at specific vertical positions on a paper strip. The interpretation of those marks as antibody reactivity to HIV proteins depends entirely on three prior assumptions, none of which the operator independently verifies:
That the antigens on the strip were derived from HIV rather than from cellular debris in the cell-culture system used to grow the alleged virus.
That the patient’s antibodies are reacting specifically to HIV-derived antigens rather than to cross-reactive cellular or microbial antigens of similar molecular weight.
That the interpretive ruleset applied to count the strip as positive corresponds to a meaningful biological state in the patient.
None of these assumptions is tested on the patient’s specimen. None can be tested by the Western blot itself. The strip records reactivity at a position. Everything else is inference downstream of the strip.
III. The cross-reactivity literature
The proteins on an HIV Western blot are produced by growing alleged HIV in cultured human cells, lysing the cell-culture preparation, and harvesting the resulting protein mixture. The preparation contains, by necessity, both viral proteins and cellular proteins of the host cell line, in proportions that vary by preparation and by manufacturer. The proteins on the strip are not purified viral antigens. They are a mixture.
Antibodies in the patient’s serum react with proteins on the strip according to molecular complementarity, not according to viral origin. An antibody raised against a cellular protein of approximately 24 kDa — present in the host cell line, in another cellular source, or generated in response to an unrelated immune stimulus — will react with any band at the 24 kDa position, whether that band is of viral or cellular origin. The Western blot does not distinguish.
Cross-reactivity at HIV Western blot band positions has been documented, in the mainstream peer-reviewed literature, by mainstream investigators, in serum from patients with the following conditions:
Pregnancy and prior pregnancy (Voevodin, Lancet 1992; PMID 1351229; see also Mortimer, Parry & Mortimer, Lancet 1985; PMID 2864587).
Recent vaccination, including influenza and tetanus vaccines (Mortimer, Lancet 1991; PMID 1671125).
Multiple transfusions and multiparous blood-product exposure (Sayre et al., Transfusion 1996; PMID 8607152).
Autoimmune disease, including systemic lupus erythematosus and rheumatoid arthritis (Esteva et al., Annals of the Rheumatic Diseases 1992; PMID 1417140).
Tuberculosis, leprosy, and other mycobacterial exposure (Kashala et al., Journal of Infectious Diseases 1994; PMID 7906291).
Malaria and other endemic infections (Biggar et al., Lancet 1985; PMID 2863543).
Liver disease and hepatic dysfunction (Mendenhall et al., New England Journal of Medicine 1986; PMID 3513019).
Recent organ transplantation (Agbalika et al., AIDS 1992; PMID 1388908).
In each condition, antibody reactivity has been observed at one or more of the band positions interpreted as HIV-positive on the Western blot. The reactivity is real. The bands appear. The interpretive question is whether the bands reflect what they are alleged to reflect.
IV. The interpretive rule is jurisdictional
A Western blot is not interpreted by the bands alone. It is interpreted by a rule — a set of criteria specifying which combinations of bands count as positive, which count as negative, and which count as indeterminate. These rules are written by national health authorities and by commercial test manufacturers. They are not standardized across jurisdictions. They have not been standardized at any point in the history of HIV diagnostic testing.
A representative summary of historical interpretive rules (compiled from CDC, MMWR 38, S-7 [1989], and Lundberg et al., JAMA 260[5] [1988]: 674–679):
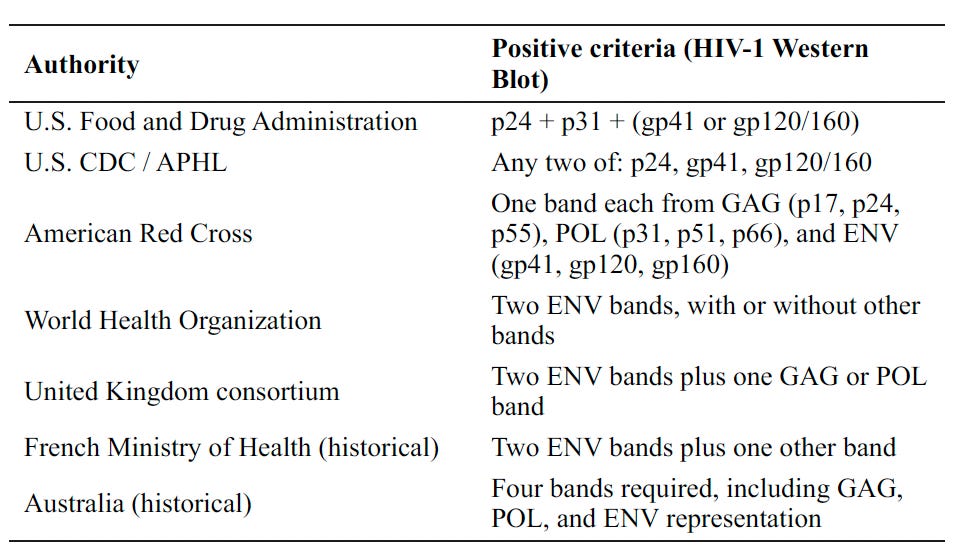
A single Western blot strip, with a single set of bands, may meet the U.S. CDC criteria for positivity, fail the Australian criteria, and fall into an indeterminate category under the WHO ruleset — simultaneously. The strip has not changed. The patient has not changed. The biology, whatever it is, has not changed. What has changed is which institutional authority is asked to read the strip.
The same blood sample, drawn from the same patient, on the same day, will return HIV-positive in one jurisdiction and HIV-negative in another.
This variability is not a marginal artifact of regulatory inconsistency. It is the operative mechanism by which a presumptive signal is converted into a diagnostic finding: the same physical evidence is interpreted to yield whatever diagnostic conclusion the local authority is prepared to support. A patient diagnosed as HIV-positive in the United States may not be diagnosable as HIV-positive in Australia using the same blood draw. The diagnostic label is jurisdictional, not biological.
V. The ELISA: the same problem, one step earlier
The ELISA (enzyme-linked immunosorbent assay) sits upstream of the Western blot in the standard testing algorithm. The industry says it detects antibodies to HIV. What it actually detects is reactivity between the patient’s serum and the same mixture of proteins harvested from the same cell-culture system used to manufacture Western blot strips. The mixture is no purer at the ELISA stage than at the blot stage. The cross-reactivity sources documented above apply to the ELISA as well, and in many cases were first documented in the ELISA literature before the Western blot was developed.
The ELISA was originally designed for blood-bank screening — to over-call positives so that no contaminated unit slipped through to a transfusion recipient. Over-calling was a feature of the design. The cost of a false positive on a blood-bank unit is that the unit is discarded. The cost of a false positive on a patient is that the patient is told he has a disease. The test was not modified when its application shifted. The same chemistry that was acceptable for screening blood units became the basis for diagnosing human beings.
VI. PCR: amplification is not demonstration
PCR is the third leg, and it operates on a different principle. PCR does not detect virus. It amplifies a selected genetic sequence — doubles whatever target is in the sample, every cycle. 30 cycles produces approximately a billion-fold copy. 40 cycles, roughly a trillion-fold. 45 cycles, approximately 35 trillion-fold.
Whatever was there originally — a fragment of replication-competent virus, a fragment of dead viral debris, a contaminant from a neighboring specimen, residual nucleic acid from a prior infection, a fragment of an endogenous retroviral sequence already present in the patient’s own genome, or laboratory background — comes out the other end looking like a positive result. The number of cycles required to produce a visible signal is called the cycle threshold, or Ct. A specimen returning positive at a Ct of 20 reflects substantial starting material. A specimen returning positive at a Ct of 38 reflects a signal that became visible only after the machine had multiplied whatever was there by roughly 300 billion. That signal may be replication-competent virus. It may equally be any of the alternatives listed above. The test does not distinguish.
The Ct value — the single piece of information that would allow the result to be interpreted — is, in standard practice, not reported on the clinical report. The clinician sees only POSITIVE.
Consider what the technique does in plain terms. Imagine a detective who claims to have recovered a suspect’s fingerprint at a crime scene. The print he produces in court, however, is not the original. It is a photocopy of a photocopy of a photocopy — run 35 times through the machine — of a single faint smudge the technician lifted from a doorknob. By the 35th copy, the smudge has become a sharp, clear, unambiguous fingerprint. The detective produces it and tells the court: that is the suspect’s print.
What the machine has done is real. The image exists. But the image’s existence does not establish what was present at the scene. The 35th copy looks the same whether the original was a fresh, complete print or a single ridge fragment from a contamination event — a passing officer, an evidence-room transfer, a smudge from yesterday’s case. The court is shown the 35th copy and told to treat it as evidence of presence. Whether the original input justified the final image is a question the photocopy itself cannot answer.
PCR works this way. The inventor of the technique was clear on the point:
“PCR is just a process that allows you to make a whole lot of something out of something. It doesn’t tell you that you are sick, and it doesn’t tell you that the thing you ended up with was really going to hurt you. With PCR, if you do it well, you can find almost anything in anybody.” — Kary B. Mullis, inventor of PCR, Nobel laureate in Chemistry, 1993 (Nobel Lecture, The Polymerase Chain Reaction, Stockholm: Nobel Foundation, December 8, 1993).
Mullis restated the point repeatedly in the decades that followed, in published interviews, recorded lectures, sworn declarations, and a long extended interview in the documentary House of Numbers (2009). He distinguished, on the record, between PCR’s value as a research tool — which he affirmed throughout his life — and its inappropriate use as a diagnostic test for active infection (Mullis, extended interview in House of Numbers: Anatomy of an Epidemic, dir. Brent Leung, 2009; Mullis, “PCR and the Myth of HIV,” Spin Magazine 1992; and Mullis’s sworn declarations in HIV-related litigation including proceedings associated with Papadopulos-Eleopulos et al. v. Perth Hospital).
The Ct problem has been documented in the peer-reviewed literature in the COVID-19 era, in studies that compared PCR positivity to viral culture infectivity. Bullard and colleagues reported that no viral growth in culture occurred at Ct values greater than 24 (Bullard et al., Clinical Infectious Diseases 71[10] [2020]: 2663–2666; PMID 32442256). Jaafar and colleagues, in the same journal a year later, reported culture positivity falling to under 3 percent at Ct greater than 35 across nearly 2,000 SARS-CoV-2 isolates; the authors recommended that patients with Ct above 33–34 should not be treated as contagious (Jaafar et al., Clinical Infectious Diseases 72[11] [2021]: e921; PMID 32986798). The Ct matters. The clinical report does not include it.
And critically: the manufacturer of the most widely deployed RT-PCR HIV-1 assay in the United States — Abbott Laboratories — states in the FDA-cleared package insert that the assay is not intended to be used as a diagnostic test to confirm the presence of HIV-1 infection. The labeling emphasizes that results are based on detection of amplified nucleic-acid signal rather than biological demonstration of a pathogen. It warns of false-positive and false-negative outcomes due to contamination, inhibition, procedural deviation, or assay limitations. It cautions that a target-not-detected result cannot be presumed to establish absence of infection (Abbott RealTime HIV-1 Package Insert, Ref. No. 6L18 / 51-602146/R6, FDA-cleared labeling).
The same manufacturer that warns, in the FDA-cleared labeling, that its assay is not a diagnostic test, has simultaneously invested in driving testing volume in targeted demographics. The Los Angeles Times reported that the;
“I Stand With Magic” campaign, a five-year, $60-million project financed by the drug firm Abbott, which makes HIV and AIDS drugs, urges blacks to be tested for HIV. Its goal is to halve the rate of new infections among U.S. blacks (Engel, “Fighting HIV with Magic,” Los Angeles Times, July 6, 2008, B1).
The campaign was launched in 2006 in partnership with Earvin “Magic” Johnson — basketball Hall of Famer and one of the most publicly visible HIV-positive figures in American life — to create educational platforms in cities with high HIV prevalence and to conduct free testing events through the Magic Johnson Foundation (Abbott Laboratories press release, “Abbott Laboratories and Earvin ‘Magic’ Johnson Announce Partnership,” April 10, 2006).
A manufacturer that pays a celebrity endorser $60 million to expand testing in a targeted population is engaged in a marketing campaign, not a public-health intervention. The test it is selling is the test its own package insert says is not a diagnostic. The endorser is a man whose continued public health is held up as evidence the test works and the treatment works.
The manufacturer says, in the package insert, that the test is not a diagnostic test. The clinician treats the result as a diagnostic test. The patient is told he has the disease.
VII. The test that is not performed
If the question is whether a particular patient harbors a particular virus, virology offers a dispositive answer. Electron microscopy (EM) visualizes viral particles directly. It does not amplify, infer, or interpret. It does not produce a signal that has to be interpreted by a ruleset. It produces an image of the particle, in the specimen, at known magnification, with measurable morphology.
EM was the technique by which every major virus of the twentieth century — poliovirus, influenza, hepatitis B, herpes simplex, measles, rabies, vaccinia — was characterized, identified, and confirmed as a discrete viral entity present in patients with the corresponding disease. It is the dispositive observational technique of twentieth-century virology.
It is not part of any routine clinical HIV diagnostic protocol. The College of American Pathologists does not require it. The Clinical and Laboratory Standards Institute does not require it. The Centers for Disease Control and Prevention’s published diagnostic algorithms do not include it. The manufacturer-recommended testing sequences for every HIV test in clinical use do not include it. The dispositive observational technique of twentieth-century virology is, in twenty-first-century clinical HIV diagnostics, structurally absent.
This absence is not contested. It is not a fringe observation. It is documentable from any clinical laboratory standards document.
The patient is never offered the test that would resolve, by direct observation, the question the antibody test poses indirectly. The diagnostic apparatus refers itself in a circle: the antibody result is confirmed by another antibody result; the amplification result is confirmed by another amplification result; the surrogate signal is confirmed by another surrogate signal. The morphological characterization of an alleged viral particle in the patient’s bloodstream is not part of the workflow at any point.
A reader is entitled to ask why. I take no position here on the answer beyond noting the structural fact: the question has not been asked, by any diagnostic protocol applied to any patient in routine clinical HIV diagnosis, and the patient has not been told that the question was available and was not asked.
VIII. The pathogenicity question that has never been answered
There is a second question, separate from the diagnostic question, that has also never been resolved in the peer-reviewed literature on the merits.
In 1987, Peter H. Duesberg — Professor of Molecular and Cell Biology at the University of California, Berkeley, an elected member of the National Academy of Sciences, the scientist who mapped the genetic structure of retroviruses and isolated the first oncogene — published a peer-reviewed article in Cancer Research titled Retroviruses as Carcinogens and Pathogens: Expectations and Reality (Duesberg, Cancer Research 47[5] [1987]: 1199–1220; PMID 3028606). The article reviewed every retrovirus known to molecular biology at that time and concluded that none had been demonstrated to cause the kind of cellular destruction that was, by then, being attributed to HIV. The article was not a polemic. It was a literature review by the field’s leading retrovirologist, published in the journal of record for cancer biology.
Duesberg restated and developed the argument in subsequent peer-reviewed papers and in his 1996 monograph Inventing the AIDS Virus (Washington, D.C.: Regnery, 1996). The institutional response was the termination of his grant funding, the loss of his graduate students, and a sustained pattern of professional exclusion — none of which engaged the argument on its merits.
To the date of this writing, the peer-reviewed literature contains no published refutation of Duesberg’s central claim that retroviruses, as a class, had not been demonstrated to cause the cytopathic effects attributed to HIV at the time the HIV hypothesis was institutionalized.
I take no position here on whether Duesberg is correct. I note only that the question he raised — whether a retrovirus is the kind of biological entity capable, by any demonstrated mechanism, of producing the immunodeficiency syndrome attributed to it — has never been answered in the peer-reviewed literature on the merits. The answer to that question is not available to the clinician informing the patient. It is not available to the patient consenting to treatment. It is not available to the prosecutor charging an HIV-exposure offense, or to the judge ruling on it. The question is formally open.
IX. The trap
The original post that prompted this essay framed the problem as a spell — modern medicine turns diagnosis into a label that, once attached, reshapes the patient’s reality. The instinct is correct. The mechanism, at the chemistry level, is what I have just described.
And the mechanism is not confined to HIV. Every infectious disease diagnosed by ELISA, Western blot, or PCR rests on the same architecture: a physical property measured (binding, weight, or amplified sequence), a disease label attached by convention, an interpretive rule that varies by jurisdiction or by laboratory, and EM structurally absent from the workflow. Every PCR-based cancer diagnosis — and these are multiplying — rests on the amplification of a sequence selected because somebody once said it was associated with malignancy, with the same Ct problem and the same gap between signal detected and disease demonstrated. The HIV literature is the most fully documented case. The structural critique is general.
The trap is not that the tests are wrong in every case. The trap is that the tests do not measure what their names assert, the interpretive rules that convert their measurements into diagnoses are written by convention and vary by jurisdiction, the one technique that could directly verify what the tests claim to find is not performed, and the underlying pathogenicity question that would tell the patient whether the diagnosis points to a real disease has never been answered in the peer-reviewed literature on the merits.
The patient is not told any of this. The clinician is not told any of this. The package insert of one of the most widely deployed tests does tell them — and is unread. The label sticks. The treatment cascade begins. The marriage, the insurance, the employment, the criminal record all reorganize around a coordinate on a gel, a binding event between unidentified molecules, and the millionfold amplification of a fragment whose origin the technique cannot determine.
That is not a diagnosis. It is a trap, built out of laboratory technique that was good enough for screening but never good enough for individual identification, granted authority no one ever asked the biology to justify.
The patient is entitled to ask the question. The clinician is entitled to ask the question. The court is entitled to ask the question. The question is this:
What was actually measured, and is that the same thing as the disease you are about to treat me for?
The forensic case-level material — the prosecutions, the testimony, the document chain — sits in the court records of the thirteen-plus litigated cases I worked between 2009 and 2015. This essay covers the laboratory architecture that produces the label. Where the cases bear directly on a specific diagnostic point, I quote the testimony and the underlying lab record directly. The architecture is the same in every case; the patient and the jurisdiction change. For the cancer-PCR companion case to this argument, see my earlier essay: When PCR Becomes a Cancer Diagnosis (rkoch.substack.com).
— Clark Baker
X: @WbClark49529 Substack: rkoch.substack.com
References
Voevodin A. “HIV screening in Russia.” Lancet 339, no. 8808 (1992): 1548. PMID: 1351229.
Mortimer PP, Parry JV, Mortimer JY. “Which anti-HTLV III/LAV assays for screening and confirmatory testing?” Lancet 2, no. 8460 (1985): 873–877. PMID: 2864587.
Mortimer PP. “The fallibility of HIV western blot.” Lancet 337, no. 8736 (1991): 286–287. PMID: 1671125.
Sayre KR, Dodd RY, Tegtmeier G, et al. “False-Positive Human Immunodeficiency Virus Type 1 Western Blot Tests in Noninfected Blood Donors.” Transfusion 36, no. 1 (1996): 45–52. PMID: 8607152.
Esteva MH, Blasini AM, Ogly D, et al. “False Positive Results for Antibody to HIV in Two Men with Systemic Lupus Erythematosus.” Annals of the Rheumatic Diseases 51, no. 9 (1992): 1071–1073. PMID: 1417140.
Kashala O, Marlink R, Ilunga M, et al. “Infection with Human Immunodeficiency Virus Type 1 (HIV-1) and Human T Cell Lymphotropic Viruses among Leprosy Patients and Contacts: Correlation between HIV-1 Cross-Reactivity and Antibodies to Lipoarabinomannan.” Journal of Infectious Diseases 169, no. 2 (1994): 296–304. PMID: 7906291.
Biggar RJ, Gigase PL, Melbye M, et al. “ELISA HTLV Retrovirus Antibody Reactivity Associated with Malaria and Immune Complexes in Healthy Africans.” Lancet 2, no. 8454 (1985): 520–523. PMID: 2863543.
Mendenhall CL, Roselle GA, Grossman CJ, et al. “False Positive Tests for HTLV-III Antibodies in Alcoholic Patients with Hepatitis.” New England Journal of Medicine 314, no. 14 (1986): 921–922. PMID: 3513019.
Agbalika F, Ferchal F, Garnier JP, et al. “False-Positive HIV Antigens Related to Emergence of a 25–30 kD Protein Detected in Organ Recipients.” AIDS 6, no. 9 (1992): 959–962. PMID: 1388908.
Centers for Disease Control. “Interpretation and Use of the Western Blot Assay for Serodiagnosis of Human Immunodeficiency Virus Type 1 Infections.” Morbidity and Mortality Weekly Report 38, S-7 (1989).
Lundberg GD. “Serological Diagnosis of Human Immunodeficiency Virus Infection by Western Blot Testing.” Journal of the American Medical Association 260, no. 5 (1988): 674–679.
Mullis KB. “The Polymerase Chain Reaction.” Nobel Lecture in Chemistry, December 8, 1993. Stockholm: Nobel Foundation. Available at: https://www.nobelprize.org/prizes/chemistry/1993/mullis/lecture/.
Mullis KB. Extended interview in House of Numbers: Anatomy of an Epidemic. Directed by Brent Leung. 2009. See also Mullis KB. “PCR and the Myth of HIV.” Spin Magazine, 1992; and Mullis’s sworn declarations in HIV-related litigation including proceedings associated with the Perth Group.
Bullard J, Dust K, Funk D, et al. “Predicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 from Diagnostic Samples.” Clinical Infectious Diseases 71, no. 10 (2020): 2663–2666. PMID: 32442256.
Jaafar R, Aherfi S, Wurtz N, et al. “Correlation between 3790 Quantitative Polymerase Chain Reaction-Positives Samples and Positive Cell Cultures, Including 1941 Severe Acute Respiratory Syndrome Coronavirus 2 Isolates.” Clinical Infectious Diseases 72, no. 11 (2021): e921. PMID: 32986798.
Abbott Molecular Inc. Abbott RealTime HIV-1 Package Insert. Reference No. 6L18 / 51-602146/R6. FDA-cleared labeling. Des Plaines, IL: Abbott Molecular.
Duesberg PH. “Retroviruses as Carcinogens and Pathogens: Expectations and Reality.” Cancer Research 47, no. 5 (1987): 1199–1220. PMID: 3028606.
Duesberg PH. Inventing the AIDS Virus. Washington, D.C.: Regnery Publishing, 1996.
Engel M. “Fighting HIV with Magic: A Growing Number of Black Leaders and Stars Try to Dispel the Fear and Stigma Surrounding Tests for the Virus.” Los Angeles Times, July 6, 2008, B1 (California / Metro Desk).
Abbott Laboratories. “Abbott Laboratories and Earvin ‘Magic’ Johnson Announce Partnership.” Press release, April 10, 2006.
— Clark Baker, 2026-05-24